In the pre-chemotherapy era of the 1960s, the
median survival of patients with metastatic breast cancer was a little
less
than two years. Since then, the greatest cancer
centers in the world have performed hundreds of prospective,
randomized clinical trials, involving tens
of thousands of patients, in an attempt to identify the best treatment
to give to the
average patient, to improve treatment outcome.
The results of these trials have been summarized by Dr. Lawrence
Shulman, of Harvard's Dana Farber Cancer Center
(click
here , reference given
here). In short, there has been not a hint
of progress, with median survivals remaining
exactly the same, just under two years.
As Shulman points
out, the implications of this are staggering. Some individual
patients are clearly and unambiguously
helped by chemotherapy. All breast cancer
oncologists have seen individual patients who had dramatic and complete
regressions of cancer and who enjoyed long
survivals. The inescapable, mathematically undeniable conclusion is clear.
Chemotherapy of metastatic breast cancer is
a zero sum game. For every month a life has been prolonged by
chemotherapy, there is another month a life
has been shortened by chemotherapy. The most likely mechanisms for this
life shortening are toxicities of the drugs
on the patient's body (such as immunosuppression and organ damage) and
the
mutagenic effects of chemotherapy on the genetically-unstable
tumor, driving the tumor into a state of more aggressive
behavior. The point is that it is not
merely a case of either being helped by chemotherapy or not being helped
by
chemotherapy. Rather, it is a case of
being helped by chemotherapy versus being killed by chemotherapy.
Not giving
toxic drugs which won't work is not abandoning
the patient to the disease, it is following the number one rule of
medicine, which is "first do no harm."
With these realities, which were clear as far
back as the 1980s, it would seem that clinical oncology investigators would
have abandoned the strategy of performing
prospective, randomized trials to identify the best treatment to give to
all
patients, and instead would have devoted most
efforts to finding ways to best match individual treatments to individual
patients. It is astonishing that this
was not done.
In November of 1999, I was, to my knowledge,
the first person to call attention to the fact that clinical oncologists
in
private practice were deriving
most of their income by running a retail pharmacy concession, in testimony
I gave to the
Medicare Executive Committee. Subsequently,
the New York Times ran an expose, and Public Interest Watch
essentially accused the American Society of
Clinical Oncology of racketeering, in its attempts to prevent reform of
the
more egregiously abusive elements of this
system (NYT and PIW articles both cited, referenced, and discussed
elsewhere on this website). Basically,
I charged that clinical oncologists shop around for the best deals on infusion
(i.v.)
chemotherapy drugs and prescribe chemotherapy,
in part, on the basis of which treatments provide them with the
greatest profit margins.
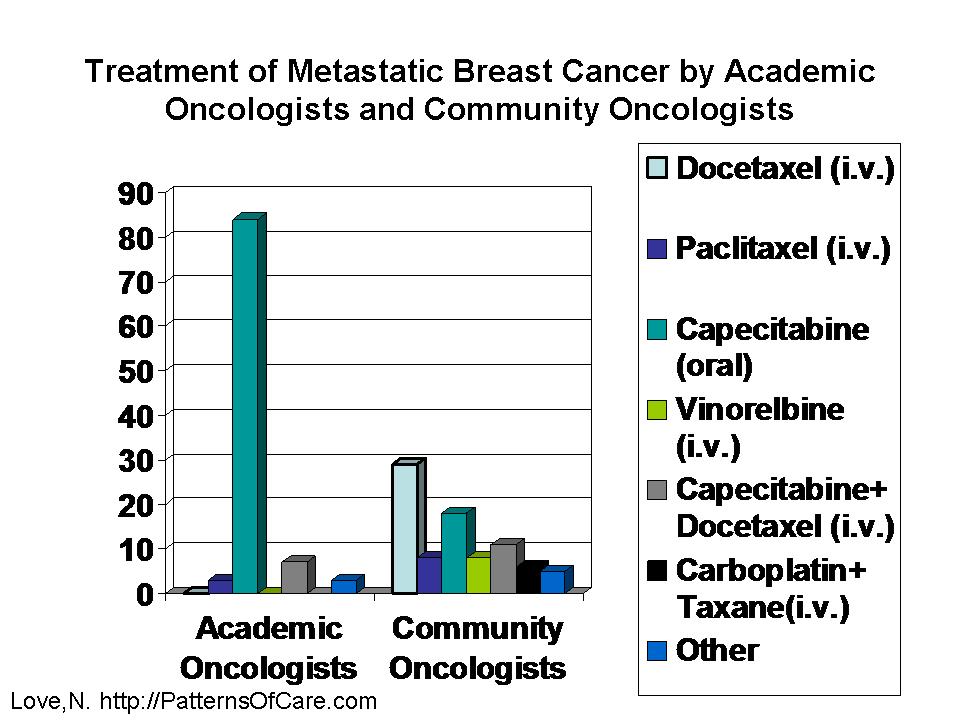
We now have proof that my charges were absolutely
correct. Neil Love, MD reports a survey of (1) breast cancer
oncologists based in academic medical centers
and (2) community based, private practice oncologists. The former
oncologists do not derive personal profit
from the administration of infusion (i.v.) chemotherapy, the latter oncologists
do
derive personal profit from infusion (i.v.)
chemotherapy, while deriving no profit from prescribing oral-dosed
chemotherapy. The results of the survey could
not have been more clear-cut. For first line chemotherapy of metastatic
breast cancer, 84-88% of the academic center-based
oncologists prescribed an oral dose drug (capecitabine), while
only 13% perscribed infusion (i.v.) drugs,
and none of them prescribed the expensive, highly remunerative drug
docetaxel. In contrast, among the community-based
oncologists, only 18% prescribed the oral dose drug
(capecitabine), while 75% prescribed infusion
(i.v.) drugs, and 29% prescribed the expensive, highly remunerative drug
docetaxel (click here
to see a graph of these data, and click here
for a link to the full text of the study [see figure 37,
volume 2, issue 1, 2005]). The existence
of this profit motive in drug selection has been one of the major factors
working against the individualization of cancer
chemotherapy based on testing the cancer biology.
The above is not to imply that the academic
oncologists are without their fair share of collective guilt. They were
misguided in not recognizing that they were
trying to fit square pegs (one size fits all treatments) into round holes
(notoriously heterogeneous diseases).
They devoted 100% of their clinical trials resources into trying to identify
the best
treatment for the average patient, in the
face of conclusive evidence that this approach was both theoretically nonsensical
and practically non-productive. Martin
Apple (of the U of Cal San Franciso) sagely noted that "any experiment
which
has failed 1000 times should be viewed with
suspicion." But the corollary is that such unsuccessful experiments
will
never be viewed as such by the thousands of
people whose careers are supported by these experiments.
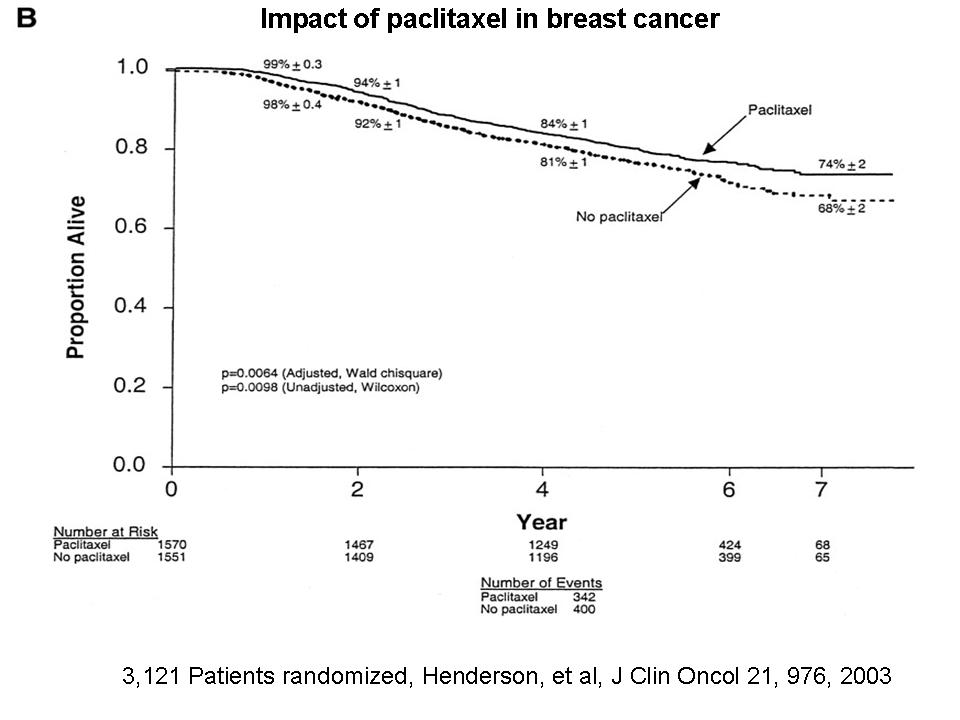
Here's an example of what passes for a successful
experiment in clinical oncology. Henderson, et al, entered 3,100
breast cancer patients in a prospective, randomized
study to compare cyclophosphamide/doxorubicin alone versus
cyclophosphamide/doxorubicin plus Taxol (in
the adjuvant, pre-metastatic setting). The results are shown on this
graph.
These results were microscopically positive,
at best, and cannot begin to justify the enormous financial and human
resources expended (while making no effort
at all to test and improve methods to individualize treatment). But
these
results changed the face of the adjuvant chemotherapy
of breast cancer. Thereafter, A/C -> Taxol became standard of
care. Taxol recently went off patent.
Now the thrust is to identify on-patent therapy which is microscopically
"better," in
ever more square peg in round hole, clinical
trials of one size fits all treatment. Already, the community-based oncologists
are migrating to A/C -> docetaxel (expensive/remunerative,
see Figure 21 in the above-quoted Neil Love study); so
what was the purpose of that 3,100 patient
prospective, randomized Henderson study?
Buyer (i.e. cancer patient) beware.
© Larry Weisenthal
April 21, 2005
{kind=link}
{kind=link}
{kind=link}
{kind=link}